Ruptured Liver Angiosarcoma: An Exceptional Complication
Salah Berkane*, Salim Belkherchi, Youcef Mahmoudi, Chemssedine Benkhelat, Djallal Hassani and Lyazid Mohamedi
Department of Surgery, Visceral and Oncological Unit, Bejaia Teaching Hospital, Algeria
*Corresponding Author: Salah Berkane, Department of Surgery, Visceral and Oncological Unit, Bejaia Teaching Hospital, Algeria.
Citation: Berkane S, Belkherchi S, Mahmoudi Y, Benkhelat C, Hassani D, et al. (2021) Ruptured Liver Angiosarcoma: An exceptional Complication. J Can Ther Res. 1(1):1-5.
Received: July 6, 2021 | Published: July 20, 2021
Copyright© 2021 genesis pub by Berkane S, et al. CC BY NC-ND 4.0 DEED. This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-No Derivatives 4.0 International License., This allows others distribute, remix, tweak, and build upon the work, even commercially, as long as they credit the authors for the original creation.
DOI: https://doi.org/10.52793/JCTR.2021.1(1)-01
Abstract
Abstract
The hemorrhage is one of serious complications of hepatic tumors It can have two causes: spontaneous or traumatic rupture or coagulopathy of consumption. The adenoma, angioma and angiosarcoma are the three kind of tumors implicated in these complications. The hemorrhage main relatively serious since it quickly involves the vital prognosis. Rupture of angiosarcoma is a rare event encountered in the daily practice. We report a case of a patient having presented this complication unfortunately with a fatal evolution.
Keywords
Hepatic angiosarcoma; Rupture; Complication
Introduction
The hemorrhage is one of serious complications of hepatic tumors. It can have several causes. The first one is a rupture secondary to traumatic origin. The second is spontaneous rupture which could start without any evident causes. The third mechanism is initiated by a phenomenom of intravascular and intratumoral consumption of elements and substances involved in coagulation or complication known as Kasaback-Merrit syndrome. The adenoma, angioma and angiosarcoma are the kind of tumor implicated in these complications [1]. The hemorrhage remains relatively serious since it quickly involves the vital prognosis. The rupture of angiosarcoma is a rare event encountered in the daily practice.
Angiosarcoma of the liver is a rare tumor, mainly of morphological diagnosis, thanks to the use of ultrasound and computed tomography. Although the majority of angiosarcoma of the liver have a benign course but worse prognosis as consequence of late diagnosis, some may be complicated by severe hemorrhage secondary to rupture. In this circumstance, the prognosis is grim, with approximately 75% of mortality [2]. We report one case with particular revolution and whose evolution was fatal.
Case Report
He is a 49-year-old man who has been complaining about symptomatically treated lipothymia for a month and a half. This patient was hospitalized for skin and mucouspallor, asthenia and lipothymia. Biological and morphological exploration was initiated in search of the etiology of this anemia in a hospital in the interior of the country. Biological examinations showed an anemia at 4.8g/100ml%, SV at 25 min the 1st hour and 60 min the 2nd hour, bilirubin at 20 mg/l, prothrombin level at 48%, blood creatinine, blood sugar, transaminases, albuminemia and cholesterolemia within normal limits. An abdominal ultrasound revealed the existence of two hepatic formations, one of 13/8 cm located at the level of the right liver and the other of 5/4 cm located at the level of the left liver. Associated with these lesions, the radiologist noted the existence of free ascites of great abundance.
The ascites puncture performed for diagnostic purposes was found to be hemorrhagic. On the basis of these results, the patient was referred to another with the diagnosis of digestive cancer at the stage of hepatic metastases and peritoneal carcinomatosis. The diagnosis is rectified at the level of the latter, after the practice of a computed tomography, which objectified images very suggestive of a giant hepatic angioma of the right liver and the left liver and peritoneal effusion evoking rather two hepatic angioma complicated by rupture than by cancer metastatic digestive. Less than 24 hours after the practice of the scanner the patient presents a severe hemorrhagic shock with distended and sensitive abdomen, an impregnable blood pressure, a pulsating pulse, sweats, a clouding and oligo-anuria. This table makes us retain the indication of an emergency laparotomy for rupture of a hepatic angioma.
After short resuscitation by filling, taking of peripheral and central venous passages a laparotomy was performed. At the opening of the peritoneal cavity, we find a hemoperitoneum of at least 4l of blood. After aspiration of the latter and pedicle clamping, temporary hemostasis was made. The exploration found an enormous ruptured tumor of the right liver at least 15cm in diameter and a second 4cm in diameter broken, also sitting astride segments II and III.
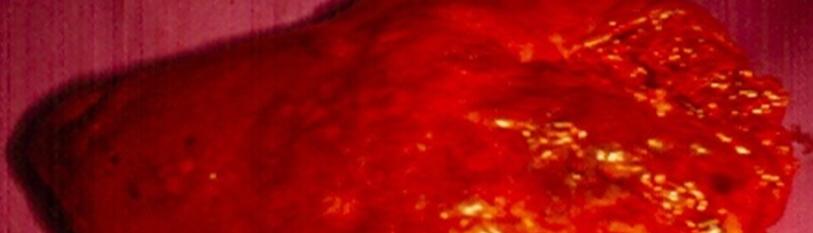
A right hepatectomy extended to segment IV is performed associated with a suture of the ruptured tumor of the left lobe. After the excision, the section of the hepatic section continues to bleed in a diffuse manner (coagulopathy) and the intervention is terminated by placing packed fields on this section section, on which the laparotomy is closed (Packing). The death occurred 3 hours after the end of the intervention by irreversible hemorrhagic shock; the hemostasis could not be made. A histological reading of the excision piece is in favor of an angiosarcoma of the liver (Figure 1, Figure 2).

Figure 1: CT Scan 15 days before tumor rupture.

Figure 2: Resected specimen.
Comments
Our rather exceptional observation illustrates the risks of angiosarcoma that are rupture and coagulopathy Kasaback-Merrit syndrome of intravascular and intratumor consumption [2,3]. It is difficult to diagnose this disease and it could be confused with hepatic angioma which has the same aspects of images on CT Scan and MRI the most appreciable exams [3]. A second interest seems to be the breaking mechanism. Trauma is a cause of rupture of the angiosarcomaas for angioma [4], but it canals occur spontaneously [5]. In our observation, the peculiarity is that the rupture was made either in two stages (minimal cracking followed by a frank rupture) or that there was a first rupture of the small angioma followed secondarily by that of the giant angioma. One can perfectly think that a cracking has occurred giving place over forty-five days to signs of anemia (pallor and lipothymia) and ascites. The frank rupture gave rise to a very serious hemorrhagic shock on the day of the intervention. This time of cracking could, in our opinion, allow establishing an adequate treatment if the diagnosis was correctly made at the beginning. We can also hypothesize, that it was the small angiosarcoma of the left liver, which ruptured at first, and that secondarily the rupture occurred at the level of the giant angiosarcomaof the right liver.
Therapeutically, the surgical sanction ranges from packing to liver transplantation. Although hepatic excision is the treatment of choice [5], it seems that embolization can lead to retrocession [6]. The period of time given by this embolization is used to correct the coagulopathy and operate outside the hemorrhagic episode and in conditions better than that of the emergency. It seems that this is not a definitive therapy because a recurrence of the hemorrhagic is always possible. The packing technique is a solution to remember in the face of a dramatic situation when the excision is risky in a hemorrhagic period, after evacuation of the effused blood.
Finally, we must take in mind, that the management of complicated angiosarcoma must be able to benefit from all therapeutic weapons [7-9]. The resection combined with chemotherapy when possible, is the most efficacious treatment for this disease nowadays [10].
Conclusion
In light of our observation and data from the literature, it seems that ruptured hepatic angiosarcoma is the complication, which is almost fatal. When the resection is possible (one site; patient in relatively good condition), it must be used with probably good results. Recognition in a patient of a clinical picture announcing acute anemia with hepatic mass or ultrasound image must raise the suspicion of the diagnosis of angiosarcoma rupture and make every effort to ensure the positive diagnosis and adopt a saving therapeutic sanction [11, 12].
References
- Chui AK, Vass J, McCaughan GW, Sheil AR. (1996) Giant cavernous haemangioma: a rare indication for liver transplantation. Aust NZJ Surg. 66(2):122-4.
- Cawich SO, Ramjit C. (2015) Herald bleeding from a ruptured primary hepatic angiosarcoma: A case report. MolClinOncol. 3(5):1063-6.
- Rujeerapaiboon N, Wetwittayakhlang P. (2020) Primary Hepatic Angiosarcoma: A Rare Liver Malignancy-Varying Manifestations but Grave Prognosis. Case Rep Gastroenterol. 14(1):137-49.
- Zhang XM, Tong Y, Li Q, He Q. (2020) Diffused hepatic angiosarcoma with Kasabach-Merritt syndrome-case report and literature review. BMC gastroenterol. 20:1-4.
- Averbukh LD, Mavilia MG, Einstein MM. (2018) Hepatic angiosarcoma: a challenging diagnosis. Cureus. 10(9): e3283.
- Hotokezaka M, Kojima M, Nakamura K, Hidaka H, Nakano Y, et al. (1996) Traumatic rupture of hepatic hemangioma. J ClinGastro-enteral. 23, 69-71.
- Tripke V, Heinrich S, Huber T, Mittler J, Hoppe-Lotichius M, et al. (2019) Surgical therapy of primary hepatic angiosarcoma. BMC surg. 19(1):5.
- Leowardi C, Hormann Y, Hinz U, Wente MN, Hallscheidt P, et al. (2006) Ruptured angiosarcoma of the liver treated by emergency catheter-directed embolization. WJG. 12(5):804.
- Timaran CH, Grandas OH, Bell JL. (2000) Hepatic angiosarcoma: long-term survival after complete surgical removal. Am Surg. 66:1153-1157.
- Almogy G, Lieberman S, Gips M, Pappo O, Edden Y, et al. (2004) Clinical outcomes of surgical resections for primary liver sarcoma in adults: results from a single centre. Eur J Surg Oncol. 30:421-427.
- OzdenI, Bilge O, Erkan M, Cevikbas U, Acarli K. (2003) Five years and 4 months of recurrence-free survival in hepatic angiosarcoma. J Hepatobiliary Pancreat Surg. 10:250-252.
- Huang NC, Kuo YC, Chiang JC, Hung SY, Wang HM, et al. (2015) Hepatic angiosarcoma may have fair survival nowadays. Medicine. 94(19).
Genesis Scientific Publication is licensed under CC BY-NC-ND 4.0![]()
![]()
![]()
![]()
